ABSTRACTS
Influence of Patient Body Weight on Probability of Return of Spontaneous Circulation Following Out-of-Hospital Cardiac Arrest: An Exploratory AnalysisAuthor: Michael W. Hubble PhD, MBA, NRP | | Associate Authors: Ginny K. Renkiewicz, PhD, Melisa D. Martin, EdD, MHS
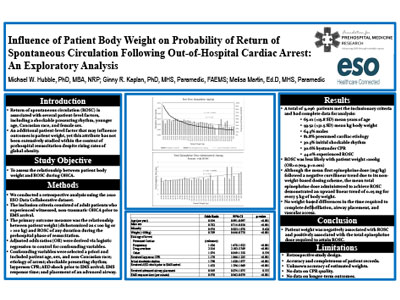
Introduction In addition to key interventions such as bystander CPR and early defibrillation, successful resuscitation of out-of-hospital cardiac arrest (OHCA) is also associated with several patient-level factors, including a shockable presenting rhythm, younger age, White race, and female sex. An additional patient-level factor that may influence outcomes is patient weight, yet this attribute has not been extensively studied within the context of OHCA despite globally increasing obesity rates. Objective To assess the relationship between patient body weight and return of spontaneous circulation (ROSC) during OHCA. Methods This retrospective study included adult patients from a national EMS electronic health record who experienced witnessed, nontraumatic OHCA prior to EMS arrival from January 2020 through December 2020. Logistic regression was used to evaluate the relationship between patient weight and ROSC while controlling for potential confounders. Results A total of 9,096 patients met inclusion criteria and had complete data for analysis. Males accounted for 64.3% of the sample, and 25.3% were minorities. The mean age of the participants was 65.01(±15.8 SD) years with a mean weight of 93.52 kg (±31.5 SD). Altogether, 81.8% of arrests were of presumed cardiac etiology, and 30.3% presented with a shockable rhythm. Layperson CPR and AED defibrillation were performed prior to EMS arrival in 30.6% and 7.3% of cases, respectively, and 44.0% experienced ROSC. ROSC was less likely with patient weight > 100 kg (OR = 0.709, p < 0.001), male sex (OR = 0.782, p < 0.001), and increasing age and EMS response time (OR = 0.994 per year, p < 0.001 and OR=0.970 per minute, p < 0.001, respectively). Patients presenting with shockable rhythms were more likely to achieve ROSC (OR = 1.790, p < 0.001) as were patients receiving layperson CPR (OR = 1.170, p < 0.001) and defibrillation prior to EMS arrival(OR = 1.658, p < 0.001). Advanced airway placement and non-White race were not predictors of field ROSC. Although the mean first epinephrine dose (mg/kg) followed a negative curvilinear trend due to its non-weight-based dosing scheme, the mean total epinephrine dose administered to achieve ROSC demonstrated an upward linear trend of 0.05 mg for every 5 kg of body weight. Conclusions Patient weight was negatively associated with ROSC and positively associated with the total epinephrine dose administered.
|